I’ve been very fortunate to have tackled quite a few complex implant cases. For me, the hardest of these is the patient missing the lower anterior incisors. This situation presents some unique challenges.
- Combination Defect. Those who have lost their lower anterior teeth typically have periodontal disease. So they have both hard tissue (bone loss) and the accompanying tissue defect.
- Aesthetics. Anytime you have to replace pink the difficulty goes up. Where to put the papillae? How to match the pink? How not to make the teeth look too long?
- Implant Positioning. These areas have minimum bone width, limited prosethetic spacing, and often have divergent roots of the neighboring canines.
Here’s an example of a such a case and how we handled it. It’s not perfect, but overall I am pleased with the result.
Jerry has been a long time patient. He lost his lower front teeth due to perio disease.

Our first order of business was to do a ‘crown down’ prosthetic approach to implant planning. I did a virtual waxup using CEREC and merged it with his CBCT.
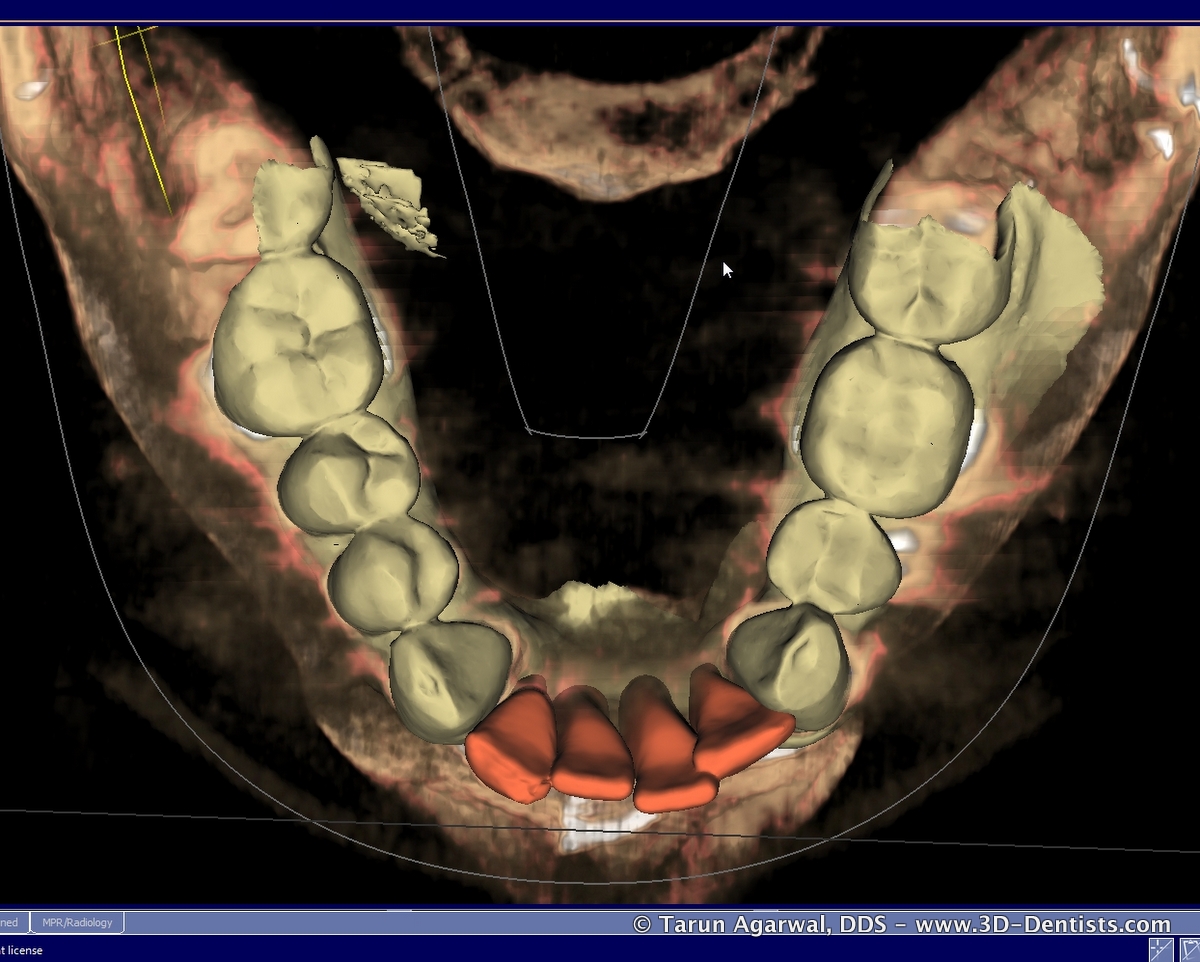
From this I was able to determine that placement in site #23 and #26 (my preferred sites) was not possible due to root divergence of the canines. Instead we needed to place implants in site #24 and #25.
Luckily, in this case there was enough bone width to avoid the need for lateral bone grafting. Even more important, we were able to plan the implants parallel.
This would give us the ability to produce a screw retained restoration with engaging abutments.


The final result is a screw retained bridge that replaces both the ‘pink’ and the ‘white’.
The final result is monolithic zirconia without any porcelain – just stain and glaze. Special thanks to Michael Keeter at Real Time Dental Lab for the lab work.

We make every effort to do nearly all our cases as screw retained restorations. Are you currenctly doing screw retained restorations? Why and why not? Please let us know in the comments section below.
Update 02/12/2016 – here is a picture of the provisional and the provisional in the mouth. As you can see i needed to adjust the provisionals in the mouth for working movements. This was then translated to the final restoration (above).