
LEVEL UP YOUR
business leadership
practice profitabilitycomplex casesdigital workflowslove for dentistrypractice culturepatient experienceteam performance
business leadership
practice profitabilitycomplex casesdigital workflowslove for dentistrypractice culturepatient experienceteam performance
From live-patient training to business coaching and team development, we’ve got everything you need to build the practice you actually want.
Join us for the ultimate dental business summit built for high-achieving dentists and their teams.
How do you want to grow?

A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.

A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.

A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.

A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.

A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.

A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.

A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.
A free space to share clinical cases, ask questions, and connect with dentists like you. Join live, no-cost events on everything from marketing strategies to clinical growth and more.

Training that supports your whole practice
Taught by real practicing dentists
Our instructors aren’t just teachers—they’re dentists in the trenches. You’ll learn proven strategies straight from professionals who understand your day-to-day challenges.
Implementation for clinical, business, and leadership growth
From case planning to team leadership, we help you learn and implement the clinical and business systems that actually move the needle in private practice.
Ongoing connection and community
You’re not in this alone. Gain access to a like-minded network of dentists and team members who share ideas, solve problems, and grow—together.
"My expectations of this mastermind group were to really find a clear path for success. I was really overworked in my practice and needed to find a way to slow down to speed up my practice."
"I think my biggest challenge prior to joining is was probably the unknown... it was a lot of just question marks, I think."
"It's hard to really dive into your practice and have someone who really knows everything about your practice and helps guide you through the challenges."
"I had had many business mentors, but what I was missing before the mastermind was that specific dental mentorship."
"The most beneficial thing outside of the all the clinical knowledge I've gained is just being around like-minded people."
Designed by dentists, for dentists
Dr. Tarun “T-Bone” Agarwal
A practicing dentist, speaker, and entrepreneur, Dr. T-Bone has helped thousands of dentists create more profitable, fulfilling practices. His practical, no-fluff approach to business and clinical growth is the foundation of everything we teach.
Dr. Sully Sullivan
A 4th-generation dentist and host of the Millennial Dentist Podcast, Dr. Sully knows what it takes to scale a modern dental practice. His passion for innovation, technology, and team leadership drives our mission to help dentists win—at work and in life.



step away to level up
Our retreat space and Dr. Sully's practice offer hands-on, distraction-free training designed to help you focus, learn, and take the next big step in your practice.
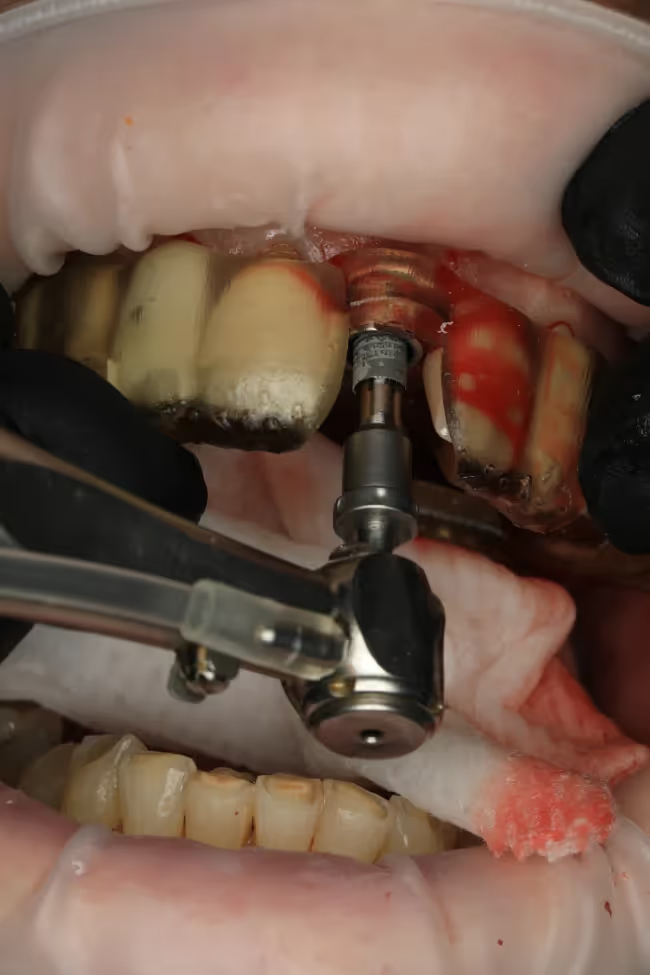
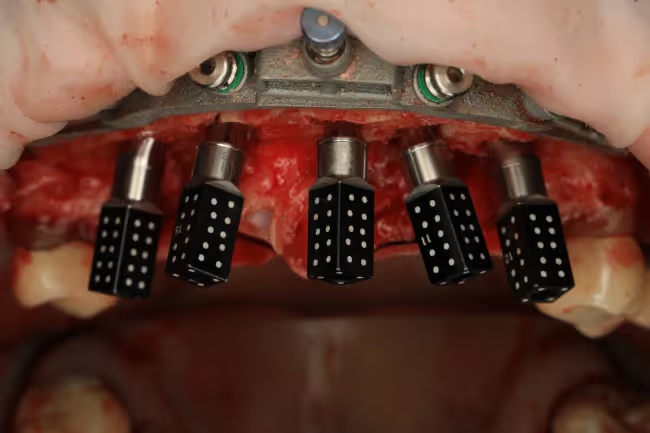
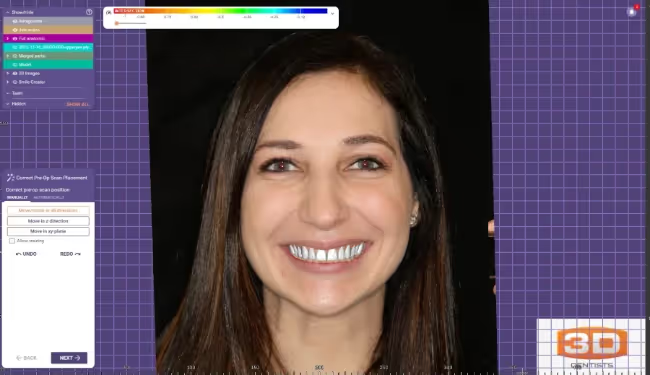
The 3D Retreat in Raleigh offers immersive learning with a high-tech training center, onsite lodging, and fully hosted meals and hospitality. The 3D Nashville Center, hosted inside Sully’s working dental office, provides live viewing of consults, surgeries, and real-time patient care for a truly immersive clinical experience.
Looking to host your event at the 3D Dentist Retreat?
Our retreat space and 3D Nashville offer hands-on, distraction-free training designed to help you focus, learn, and take the next big step in your practice.

Join us for the ultimate dental business summit built for high-achieving dentists and their teams. Walk away with proven strategies to increase revenue, reduce stress, and lead with confidence.
- Boost productivity, profitability, and team performance—without burning out
- Get real-world strategies on business, finances, and leadership
- Learn directly from dentists and teams who’ve done it successfully
- Early registration includes one Universal Studios park ticket
3D Growth Summit
Dr. Sully Sullivan
+ more